Nighttime GERD & Sleep Apnea: The Hidden Bidirectional Connection That Makes Both Worse
Nighttime GERD & Sleep Apnea: The Hidden Bidirectional Connection | HealthGuide
HealthGuideHome› Digestive Health› GERD Sleep Risks› GERD & Sleep Apnea
Back to: Can You Die From Acid Reflux in Your Sleep?
If you have acid reflux and snore at night, you may have two conditions secretly amplifying each other, and treating only one won’t fix either.
Updated April 2026· 3,400 words·8 min read·Medically reviewed
You’ve been managing your acid reflux for years. You take your medication, you avoid the trigger foods, and you try to eat dinner early. But every morning, you still wake up with a raw throat, a nagging cough, and a tiredness that sleep doesn’t fix. Sound familiar?
If it does, there’s a question your gastroenterologist might not have asked yet: do you snore?
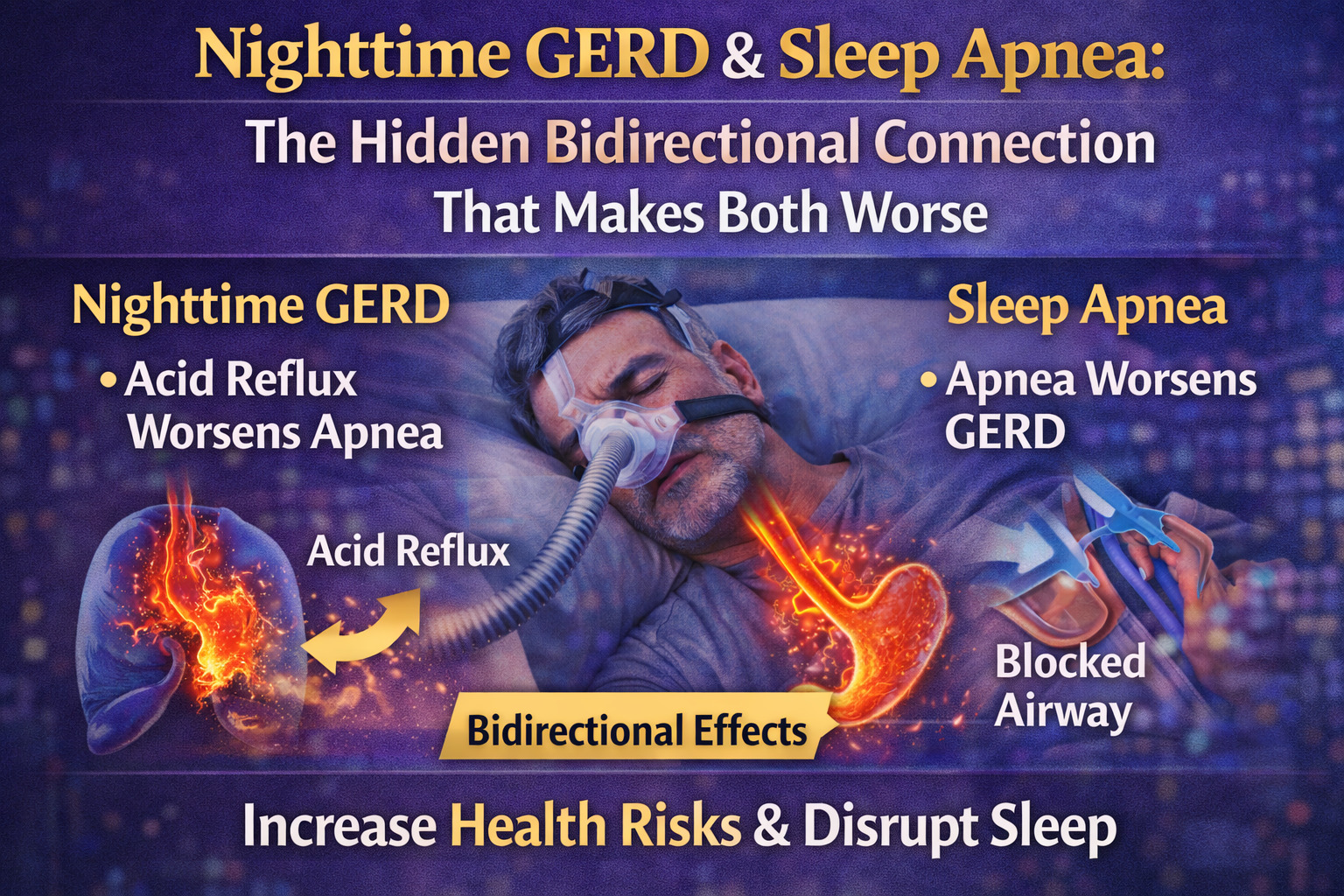
The link between obstructive sleep apnea (OSA) and gastroesophageal reflux disease (GERD) is one of the most clinically significant and most underdiagnosed relationships in sleep medicine. These aren’t just two conditions that happen to coexist in the same patient. They have a bidirectional, mutually reinforcing relationship where each condition actively makes the other worse. When both are present simultaneously, the risk for nighttime aspiration, esophageal damage, and chronic respiratory complications rises substantially.
This article unpacks the mechanism, the research, and critically, what you should do about it. If you haven’t read the main pillar article on nighttime GERD risks yet, that’s a good starting point. This piece goes deeper into a specific dimension of that picture.
Quick Answer
Do GERD and sleep apnea make each other worse? Yes, in a bidirectional, reinforcing cycle. During obstructive sleep apnea events, the body creates powerful negative intrathoracic pressure trying to force air past the obstruction, which literally suctions gastric acid upward into the esophagus. Conversely, acid reaching the throat can trigger laryngospasm (vocal cord closure) that interrupts breathing and worsens OSA. Studies show CPAP therapy for sleep apnea reduces GERD symptom frequency and severity. Both conditions must be identified and treated for either to be well-controlled.
~60%of patients with OSA report frequent GERD symptoms
3–4×higher GERD prevalence in OSA patients vs. general population (research estimates)
50%aspiration event rate in stroke patients, illustrating how impaired reflexes + GERD combine
CPAPshown in multiple studies to reduce acid reflux severity as a secondary benefit
How Sleep Apnea Drives Acid Reflux: The Vacuum Mechanism
To understand why these two conditions interact so dramatically, you need to understand what physically happens during an obstructive sleep apnea event because it’s counterintuitive.
In OSA, the upper airway collapses during sleep. Your diaphragm and chest muscles keep contracting, trying to breathe, but the airway is blocked. The result: your chest is creating a powerful negative pressure, essentially a vacuum, trying to suck air through an obstruction.
Here’s the problem. The same negative pressure that’s trying to pull air into your lungs is also acting on everything above your diaphragm. Including your stomach. Including the gastroesophageal junction, the doorway between your stomach and esophagus, the lower esophageal sphincter (LES) is supposed to stay closed.
That suction force can transiently overcome the LES pressure, pulling gastric contents upward into the esophagus. This is called pressure-induced gastroesophageal reflux, and it’s a distinct mechanism from the typical GERD reflux caused by a chronically weak or relaxed LES. What makes it particularly insidious is that it can occur multiple times per hour in moderate-to-severe OSA, with each apnea event potentially triggering a reflux episode.
The OSA → GERD Cascade
→ Airway collapses during sleep
→ Diaphragm creates negative pressure
→ Suction overcomes LES
→ Acid enters esophagus
→ Tissue damage + awakening
And it doesn’t stop there. The acid that enters the esophagus during an apnea event can travel all the way to the larynx and throat, a condition called laryngopharyngeal reflux (LPR). When acid reaches the vocal cords, it can trigger laryngospasm: a reflexive, protective closure of the vocal cords to prevent aspiration. Laryngospasm itself stops breathing. So acid reflux triggered by an apnea event can cause its own apnea-like breathing interruption in return.
This is the bidirectional loop: apnea drives reflux, reflux drives airway obstruction, airway obstruction drives more apnea. In patients with both conditions, you’re not dealing with a simple addition of two problems; you’re dealing with an amplification cycle.
How Acid Reflux Makes Sleep Apnea Worse
The reverse pathway is equally important to understand, because it explains why some OSA patients have disproportionately severe or difficult-to-treat sleep apnea.
Airway Inflammation from Chronic LPR
Chronic laryngopharyngeal reflux, acid repeatedly reaching the throat and larynx, causes inflammation and edema (swelling) of the upper airway tissues. The throat is not designed to handle acid. Unlike the stomach lining, it has no protective mucus layer. Even small amounts of acid cause irritation, and chronic exposure causes ongoing tissue inflammation.
Swollen, inflamed upper airway tissues are more prone to collapse during sleep. This is one mechanism by which chronic GERD can worsen the severity of OSA over time, gradually narrowing and softening the airway structures that are supposed to maintain patency during sleep.
Laryngospasm-Induced Apnea Events
As described above, acid reaching the vocal cords can trigger laryngospasm. This manifests in the sleep study record as an apnea event, but it’s caused by a reflex airway closure rather than the passive tissue collapse typical of conventional OSA. These events may not respond as well to CPAP therapy alone if the underlying acid reflux isn’t also controlled.
This is clinically important: a patient with both conditions who’s on CPAP but still having frequent respiratory events or morning symptoms may be having laryngospasm events driven by uncontrolled reflux, and treating only the apnea without addressing the GERD leaves a meaningful driver of symptoms untouched.
The Obesity Amplifier
Both GERD and OSA are independently associated with obesity. Excess abdominal fat increases intra-abdominal pressure (worsening GERD), while excess oropharyngeal fat deposits narrow the upper airway (worsening OSA). In obese patients, both conditions are often more severe, more closely linked, and more responsive to weight loss as a treatment than in non-obese patients. Even a 10% reduction in body weight has documented benefits for both GERD severity and OSA severity.
🔬 Research Context
The relationship between OSA and GERD has been studied in multiple controlled trials. A systematic review in gastroenterology literature found GERD prevalence significantly higher in OSA patients than in matched controls. Mechanistic studies using simultaneous polysomnography (sleep study) and esophageal pH monitoring have confirmed that many reflux events in OSA patients occur in temporal proximity to apnea events, supporting the negative-pressure mechanism. See related NLM research on GERD and respiratory conditions.
CPAP Therapy and GERD: What the Evidence Shows
Here’s the most clinically useful finding from this area of research: treating OSA with CPAP appears to reduce GERD symptom burden as a secondary benefit, even in patients who haven’t changed their diet, medications, or other GERD risk factors.
The mechanism makes sense. CPAP delivers positive airway pressure that prevents the upper airway from collapsing. This eliminates the negative intrathoracic pressure swings that pull acid upward. When the vacuum mechanism is abolished, the pressure-induced component of reflux disappears.
Multiple studies have documented this effect. Patients with both OSA and GERD who start CPAP therapy report fewer nocturnal reflux episodes, reduced heartburn frequency, and in some cases, reduced need for antacid medications. The improvement in GERD symptoms isn’t universal; patients with GERD driven primarily by a chronically weak LES (rather than pressure-induced mechanisms) may see less benefit, but it’s well-documented in the OSA-dominant patient profile.
“The temporal relationship between apnea events and acid reflux episodes in concurrent pH-impedance and polysomnography studies demonstrates clearly that airway obstruction is an independent driver of nocturnal GERD in many patients. This has practical implications: CPAP should be considered part of the reflux treatment strategy in patients with documented OSA.”
Synthesized from gastroenterology and sleep medicine clinical literature on GERD-OSA comorbidity, referencing concurrent pH monitoring and polysomnography study designs
What This Means Practically
If you’re being treated for GERD but continue to have significant nighttime symptoms despite appropriate medication and lifestyle interventions, and you haven’t been screened for sleep apnea, ask your doctor about a sleep study. The symptoms overlap enough that each can mask the other:
- Waking up with a wet cough can be aspiration from reflux or partial airway obstruction from OSA or both
- Morning headaches can indicate nocturnal hypoxia from OSA or poor sleep quality from GERD
- Unrefreshing sleep despite adequate duration is a hallmark of OSA, but GERD-induced night waking produces the same complaint.
- Chronic throat clearing and hoarseness fit LPR from GERD and upper airway inflammation from OSA equally
The diagnostic overlap is real. A sleep study (polysomnography or home sleep apnea test) resolves the question. If OSA is confirmed, CPAP therapy often produces improvements in both conditions simultaneously.
How the Combination Elevates Aspiration Risk
Recall from the pillar article that aspiration of stomach contents entering the lungs is the most direct mechanism by which nighttime GERD can become dangerous. The OSA-GERD combination is particularly concerning for aspiration because it combines:
- More frequent reflux events (pressure-induced reflux during apnea)
- Larger reflux volumes (negative pressure events can produce high-volume reflux)
- Impaired arousal response, OSA patients have altered arousal thresholds; they may not fully wake to clear an airway insult as quickly.
- Upper airway inflammation from LPR, reducing mucociliary clearance efficiency
In a healthy person with mild, occasional GERD, the body’s aspiration defenses, cough reflex, laryngospasm, and mucociliary clearance handle minor aspiration events routinely. But the OSA-GERD combination stresses each of these defenses simultaneously while also generating more frequent and larger reflux events to defend against.
This is especially relevant in elderly patients, patients with any neurological impairment, and patients who use sedating medications (sleep aids, antihistamines, opioids, benzodiazepines), all of which suppress the protective reflexes that normally catch aspiration before it reaches the lungs.
🚨 High-Risk Combination to Flag for Medical Evaluation
- Untreated or undertreated OSA + chronic GERD + any of the following:
- Age 65+
- Nighttime sedative use (sleep aids, antihistamines, opioids, benzodiazepines)
- History of stroke or neurological disorder affecting swallowing
- Recurrent respiratory infections or unexplained chronic cough
This combination profile represents significantly elevated aspiration risk. Proactive evaluation by both a gastroenterologist and a pulmonologist or sleep specialist is warranted.
Getting the Right Diagnosis: What Testing Looks Like
The good news about this area is that the diagnostic tools are well-established. The challenge is that diagnosing the OSA-GERD combination requires going to two different specialists, which doesn’t always happen systematically. Here’s what comprehensive evaluation looks like:
For Sleep Apnea
- Screening questionnaire The Epworth Sleepiness Scale and STOP-BANG questionnaire are validated screening tools your doctor can administer in-office. They assess snoring, daytime sleepiness, witnessed apneas, blood pressure, BMI, age, neck size, and sex to calculate OSA risk.
- Home sleep apnea test (HSAT). For patients with high pre-test probability and no complex comorbidities, a home sleep test, a portable device worn overnight, can diagnose OSA. It measures breathing effort, airflow, oxygen saturation, and heart rate.
- In-lab polysomnography The gold standard. Monitors brain waves, eye movements, muscle activity, heart rate, breathing effort, airflow, and oxygen levels simultaneously. More comprehensive than home testing and required for complex cases or when home testing is inconclusive.
For GERD Severity Assessment
- Upper endoscopy (EGD) Direct visualization of the esophageal lining. Identifies esophagitis, ulcers, Barrett’s esophagus, strictures, and hiatal hernia. Recommended for patients with GERD symptoms for 5+ years, alarm symptoms (dysphagia, weight loss), or inadequate symptom control on medications.
- 24-hour pH-impedance monitoring The most accurate test for quantifying reflux. A thin catheter placed in the esophagus measures acid exposure over 24 hours while you go about your normal activities. Crucially for OSA patients, this test can be correlated with sleep study data to document the temporal relationship between apnea events and reflux episodes.
- Esophageal manometry Measures the pressure and coordination of esophageal muscle contractions and LES pressure. Useful when surgical treatment is being considered or when motility disorders are suspected alongside GERD.
Treating Both Conditions: A Coordinated Approach
The key insight here is that these conditions share several risk factors and lifestyle drivers, which means lifestyle interventions address both simultaneously. And where medical treatments are needed, the sequencing matters.
| Intervention | Benefit for GERD | Benefit for OSA | Priority Level |
|---|---|---|---|
| Weight loss (10%+ of body weight) | Reduces intra-abdominal pressure; improves LES tone | Reduces oropharyngeal fat; dramatically improves AHI in many patients | High – addresses both simultaneously |
| CPAP therapy for OSA | Eliminates pressure-induced reflux mechanism; documented GERD symptom improvement | Gold standard for moderate-severe OSA | High – start immediately if OSA diagnosed |
| Eliminate alcohol before bed | Prevents LES relaxation; reduces acid volume | Alcohol worsens muscle tone in upper airway; worsens apnea severity | High – clear benefit for both |
| Left-side sleeping, head elevation | Strong evidence for reducing nighttime reflux | Side sleeping reduces OSA severity in many patients (positional OSA) | High – free, immediate benefit |
| PPI therapy (proton pump inhibitors) | Reduces acid secretion; standard GERD treatment | Indirect benefit: less acid reaching throat reduces laryngeal inflammation | Medium – manage with physician |
| Avoid eating within 3 hours of sleep | Allows gastric emptying before lying down | Reduces aspiration risk during OSA events | Medium – important, especially for obese patients |
| Oral appliance therapy for OSA | Less mechanical advantage than CPAP for pressure-induced GERD, but still helps | Effective alternative to CPAP for mild-moderate OSA and CPAP-intolerant patients | Medium – discuss with sleep specialist |
| Surgical GERD treatment (fundoplication) | Mechanically reinforces LES; durable long-term efficacy | Indirect benefit by eliminating LPR-driven airway inflammation | Low (selected patients only) -specialist decision |
The Sequencing Recommendation
When both conditions are confirmed, the general approach in clinical practice is:
- Start CPAP therapy for OSA promptly – this has direct, near-immediate effects on pressure-induced GERD
- Continue or optimize GERD medication management in parallel (don’t wait to see if CPAP “fixes” the GERD – manage it actively from both sides)
- Implement shared lifestyle changes (weight loss if applicable, alcohol elimination, sleep positioning) as a foundation
- Reassess GERD symptoms after 4–8 weeks of effective CPAP therapy – some patients find significant reduction and may be able to step down medication under physician guidance
- Consider specialist referral (gastroenterology + pulmonology or sleep medicine) if either condition remains poorly controlled on this approach
✅ Practical Takeaway
If you have diagnosed GERD and you snore loudly, wake up unrefrested, or have daytime sleepiness: ask your primary care doctor for an OSA screening and, if indicated, a sleep study. Getting an OSA diagnosis and starting CPAP may produce a meaningful improvement in your reflux that years of dietary adjustments and antacids alone couldn’t achieve. The Sleep Foundation provides accessible information on OSA screening and treatment options.
Frequently Asked Questions
Does CPAP help with acid reflux?
Yes, in patients where OSA is driving pressure-induced reflux episodes. CPAP eliminates the negative intrathoracic pressure swings that pull acid upward during apnea events. Multiple studies document GERD symptom reduction as a secondary benefit of CPAP therapy. The benefit is most pronounced for patients with moderate-to-severe OSA those having many events per hour.
Can acid reflux cause sleep apnea?
Acid reflux can worsen existing OSA through two mechanisms: (1) laryngopharyngeal reflux causes airway tissue inflammation and edema, narrowing the upper airway and making it more collapsible; (2) acid reaching the vocal cords triggers laryngospasm, which produces breathing interruptions that appear similar to apnea events on a sleep study. Whether GERD alone can cause OSA in someone without any other risk factors is less established, but it’s clear that chronic reflux can worsen the severity of pre-existing OSA.
What are the symptoms of nighttime GERD combined with sleep apnea?
Overlapping symptoms include: waking up with a wet cough, sore throat, or burning sensation; waking up gasping or feeling short of breath; morning hoarseness or voice changes; unrefreshing sleep despite adequate hours; daytime fatigue and cognitive fog; frequent nighttime awakenings; acid taste or regurgitation at night. The difficulty is that these symptoms don’t tell you whether OSA, GERD, or both are driving them, which is why objective testing (sleep study + pH monitoring) is often needed for a clear diagnosis.
Is it dangerous to have both GERD and sleep apnea untreated?
Having both conditions untreated carries compounded risks. Untreated OSA is independently associated with cardiovascular risk (hypertension, arrhythmia, stroke). Untreated GERD risks esophageal damage, Barrett’s esophagus, and aspiration pneumonia. When both are present simultaneously, the aspiration risk is elevated because OSA produces more frequent, higher-volume reflux events while also potentially impairing the arousal response needed to prevent aspiration. For elderly patients, those with neurological conditions, or those on sedating medications, the combination warrants prompt evaluation and treatment.
Can weight loss resolve both GERD and sleep apnea?
Weight loss is one of the few interventions with strong evidence for meaningful benefit in both conditions simultaneously. For OSA, a 10–15% body weight reduction can reduce the apnea-hypopnea index (AHI) by 25–50% in some patients with weight-related OSA. For GERD, even modest weight loss reduces intra-abdominal pressure, improves LES tone, and is associated with significant symptom improvement. Bariatric surgery in severely obese patients has been associated with near-complete resolution of both conditions in some cases. Weight management should be a cornerstone of treatment for any patient with BMI ≥ 30 and either condition.
Related Articles in This Series
- Can You Die From Acid Reflux in Your Sleep? – Pillar page covering all nighttime GERD risks, complications, and prevention
- Barrett’s Esophagus: The GERD Complication Every Long-Term Sufferer Needs to Understand
- Aspiration Pneumonia: When Acid Reflux Reaches Your Lungs
- The Best Sleeping Position for Acid Reflux: What the Research Actually Shows
Medical Disclaimer: This article provides general health information only and is not a substitute for professional medical advice, diagnosis, or treatment. Consult a qualified healthcare provider for personal medical guidance.
External References:
- Sleep Foundation – Obstructive Sleep Apnea Overview
- National Library of Medicine – GERD and Respiratory Tract Disorders (clinical review)
- American College of Gastroenterology – GERD Resources
- NIDDK – GERD in Adults
- American Academy of Sleep Medicine – CPAP therapy efficacy studies and OSA comorbidity data
- Katz PO, Gerson LB, Vela MF: ACG Guidelines for GERD Diagnosis and Management (referenced throughout)
- Respiratory Therapy Journal: Acid Aspiration – Inflammation and Resolution (clinical studies on aspiration mechanisms during sleep)
Last updated: April 2026.