What Is Autologous Blood Transfusion? A Complete Medical Guide (2026)
For most people, “blood transfusion” means one thing: a bag of someone else’s blood going into your arm. But there’s a second, medically distinct option that’s been quietly used in operating rooms since the 1970s and has just moved from the footnotes to the headlines.
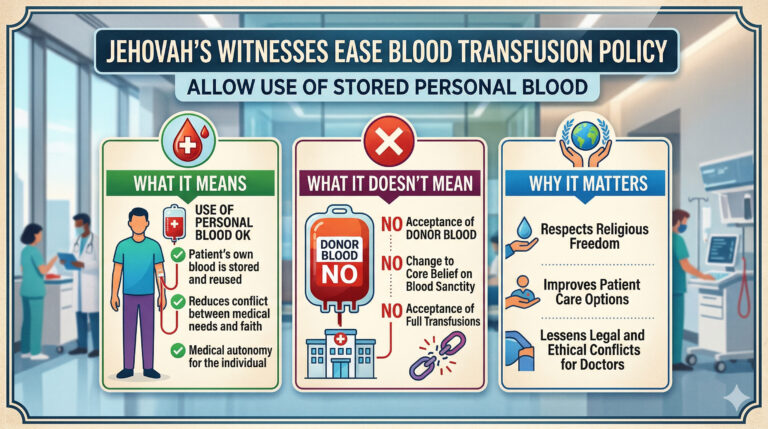
Jehovah’s Witnesses Ease Blood Transfusion Policy: Full Explainer
When the Governing Body of Jehovah’s Witnesses announced in March 2026 that members could now store and reuse their own blood during scheduled procedures, millions of people suddenly needed to understand a medical technique they’d never heard of. Autologous blood transfusion, the practice of receiving your own pre-stored or intraoperatively collected blood, is now a personal conscience choice for 9.2 million Jehovah’s Witnesses worldwide.
So what exactly is it? How does it work? Who is it for? And what are the real risks?
Autologous Blood Transfusion: The Snapshot Definition
Autologous blood transfusion is a medical procedure in which a patient receives their own blood during surgery to replace blood lost during the procedure. It works by collecting a patient’s blood before or during a procedure, storing or processing it, and reinfusing it back into the same person’s circulatory system. Unlike standard transfusions, there is no donor. The patient and the donor are the same individual.
This eliminates two of the biggest risks associated with donor blood: immune reaction, where the recipient’s body attacks foreign blood cells, and disease transmission, including HIV, hepatitis B and C, and other bloodborne infections. For this reason, autologous transfusion has been increasingly valued in surgical medicine independent of any religious framework.
The Three Types: How Each One Works
Not all autologous transfusions are the same. There are three distinct methods, each with different timing, mechanics, and clinical applications.
1. Preoperative Autologous Donation (PAD)
This is the method now permitted under the updated Jehovah’s Witness policy, and the one most patients picture when they hear “bank your own blood.”
The process works like this. Weeks before a scheduled surgery, the patient donates one or more units of their own blood, typically at a hospital blood bank. That blood is stored, labeled exclusively for their use, and made available on the day of surgery. If blood loss during the operation exceeds what the body can sustain, the stored blood is transfused back.
According to research published in PMC and NIH, repeated pre-surgical autologous donation can stimulate bone marrow cell proliferation and red blood cell regeneration, potentially improving hematopoietic recovery after surgery compared to patients who receive donor blood.
Practical requirements:
- Minimum 3 to 4 weeks before surgery
- Most programs require donations to be completed at least 3 days before the operation
- Patient must be medically eligible, evaluated for the likelihood of needing blood, and have underlying conditions
- The facility must have an established autologous donor program
- Any unused blood is discarded after the patient is discharged; it cannot be donated to others
Who benefits most: Patients undergoing elective orthopedic surgery, cardiovascular procedures, or surgeries with predictable blood loss.
Key limitation: This method only works when surgery is planned in advance. In an emergency, PAD is not applicable.
2. Acute Normovolemic Hemodilution (ANH)
This technique is performed in the operating room on the day of surgery, immediately before the procedure begins.
The process involves withdrawing blood from the patient, typically 1 to 3 units, and replacing it with fluids to maintain blood volume. During surgery, the patient’s blood becomes diluted. This means less red blood cell loss occurs during bleeding. After the procedure, the stored blood is returned to the patient.
Advantages:
ANH does not require advance planning or blood bank storage.
Limitations:
Temporary dilution reduces oxygen-carrying capacity, which must be carefully monitored.
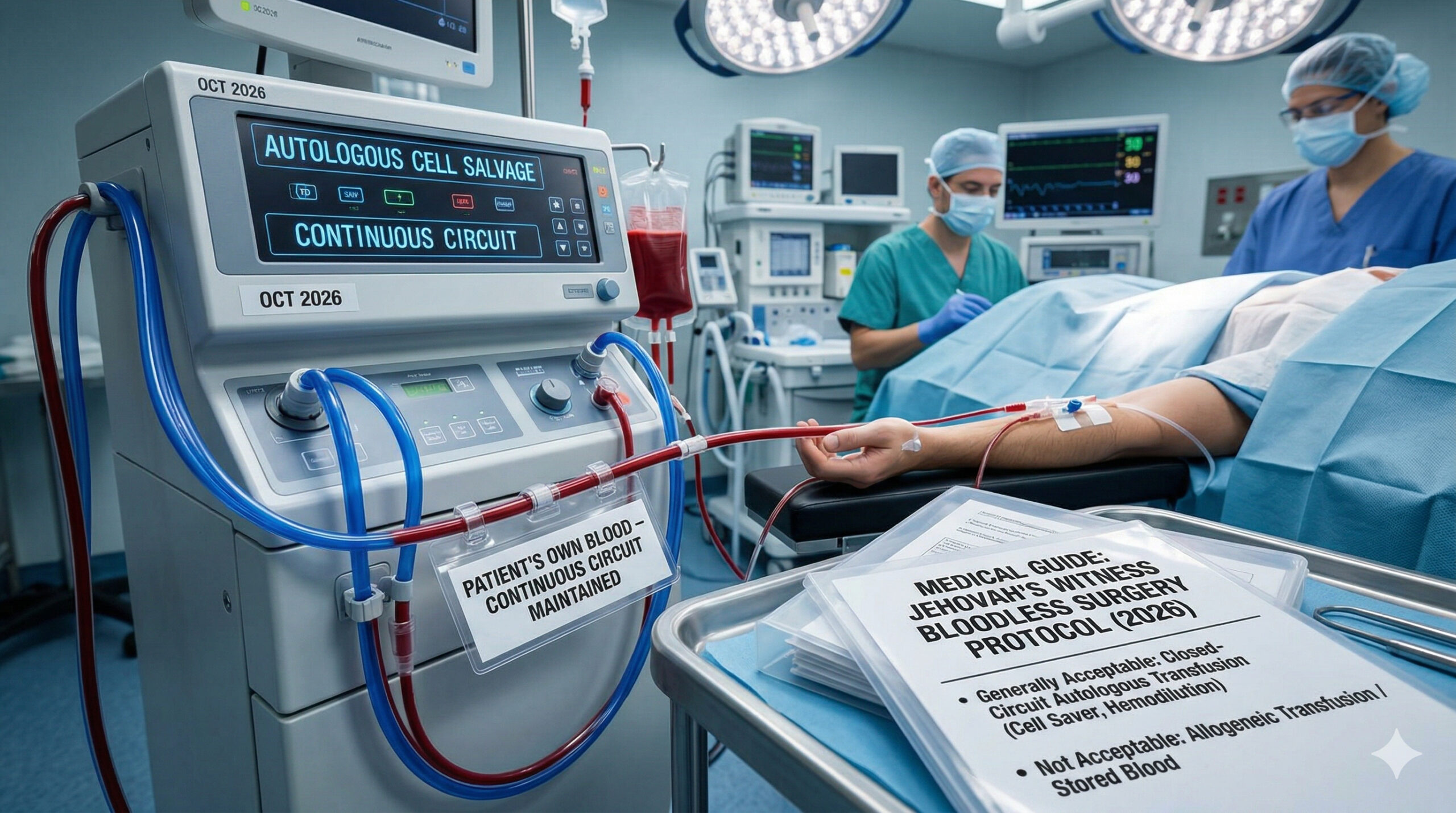
3. Intraoperative Cell Salvage (ICS), Also Called Cell Saver
Rather than collecting blood before surgery, ICS collects blood during surgery as it is shed into the operative field.
A specialized machine sucks blood, washes and concentrates the red blood cells, and reinfuses the cleaned blood back into the patient in near real time.
Researchers estimate that using cell salvage in surgeries with expected blood loss exceeding one liter could save thousands of blood units annually in healthcare systems.
Important note for Jehovah’s Witness patients:
Many individuals had already accepted cell salvage using a continuous closed-circuit system. The key distinction was that blood remained in continuous contact with the body. The new policy specifically addresses blood storage.
What Surgeries Use Autologous Transfusion?
The short answer: many surgical specialties rely on it.
Cardiovascular surgery
Coronary artery bypass, valve replacement, and aortic procedures routinely use cell salvage.
Orthopedic surgery
Joint replacements, spinal fusion, and reconstruction surgeries frequently use autologous techniques.
Neurosurgery
Precision procedures reduce the risk of immune reaction.
Cancer surgery
Complex tumor removal surgeries may involve autologous transfusion when large blood loss is expected.
Obstetric surgery
Autologous transfusion has been used in severe obstetric hemorrhage cases.
The Risk Profile: Honest Numbers
Autologous transfusion is generally safer than donor transfusion in several areas, but it is not risk-free.
Lower risks compared to donor blood:
- No blood type incompatibility reactions
- No transmission of major viral infections
- Reduced immune complications
- Reduced immunosuppressive effects
Risks specific to autologous transfusion:
- Wrong-unit administration, which is rare
- Temporary reduction in clotting factors
- Reduced platelets in some procedures
- Theoretical risk of reinfusing cancer cells in oncology surgery
Overall assessment:
Medical literature consistently shows strong safety performance for autologous transfusion, particularly with modern monitoring and protocols.
Autologous Transfusion and the Jehovah’s Witness Context: What Changed and What Did Not
This section is specifically relevant to Jehovah’s Witness patients and families.
The March 2026 announcement reclassified preoperative blood storage as a personal medical decision.
What this means practically:
- Patients may now choose to store their own blood before elective surgery
- The decision is voluntary
- Medical directives may need updating
What has not changed:
- Receiving donor blood remains prohibited under the current doctrine
- Emergency situations remain medically challenging
- Policies regarding minors remain unchanged
A Brief History: How Autologous Transfusion Developed
The first documented use of self-donated blood occurred in 1818 during the treatment of postpartum hemorrhage. Modern autologous transfusion programs expanded significantly during the late twentieth century as blood safety concerns increased.
Technological advances, particularly the development of automated cell salvage machines, made the practice safer and more efficient. Today, autologous transfusion is considered a standard component of modern surgical care in many hospitals.
Frequently Asked Questions
How far in advance do I need to donate my blood?
Most programs begin 4 to 6 weeks before surgery.
Does this work in emergencies?
No. Preoperative donation requires planning.
Is autologous transfusion covered by insurance?
Coverage varies depending on country, insurer, and medical necessity.
Can anyone donate their own blood?
No. Eligibility depends on medical evaluation and overall health status.
Is autologous transfusion completely risk-free?
No medical procedure is completely risk-free, but risks are generally lower than those of a donor transfusion.
Key Resources
- Pillar Page: Jehovah’s Witnesses Ease Blood Transfusion Policy Full Explainer
- Autotransfusion Wikipedia
- Autologous Blood Transfusion PubMed
- British Journal of Anaesthesia Education Autologous Blood Transfusion
Medical disclaimer:
This article is for informational purposes only and does not constitute medical advice. Always consult a licensed physician before making decisions about surgical preparation or medical procedures.